AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2690-4861/022
*Corresponding Author: Jochanan E. Naschitz, Bait Balev Nesher, Department of geriatric and palliative care, and The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Citation: Jochanan E. N, Segal G, Zaygraykin N, Starikov N, Leibovitz G. (2020) Calf Pressure Ulcers: Facts Defying the Prevailing Concept. International Journal of Clinical Case Reports and Reviews. 3(1); DOI: 10.31579/2690-4861/022
Copyright: © 2020 Jochanan E. Naschitz, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 March 2020 | Accepted: 04 July 2020 | Published: 08 July 2020
Keywords: Calf Pressure Ulcers; pathophysiology
Background According to the classical concept the capillary closing pressure is 30-32 mmHg and the calf interface pressure is 10-20 mmHg. So, pressure ulcers cannot occur on the calf. Observations from the bedside oppose the concept.
Aim To examine the features and clinical context of what appear to be calf pressure ulcers.
Design Prospective observational study in a long-term geriatric and palliative care unit.Methods Guideline directed diagnosis and treatment of skin ulcers.
Results
Six out of 1631 patients newly admitted to our institution during a 15 month period had skin ulcers on their calves, resembling typical pressure ulcers. In four patients the calf ulcers evolved concurrently with pressure ulcers at other sites. Two patients had a single calf ulcer and no other pressure ulcer. By the ulcers' location, the clinical context and the normal appearance of the adjacent skin, the calf ulcers differed from venous, ischemic, neuropathic and vasculitic ulcers. Except for their elongated shape, contrasting to the round shape of pressure ulcers at other sites, the calf ulcers were similar to typical pressure ulcers. Calf pressure ulcers have been ignored in the literature, maybe as a consequence of the longtime dominant theory concerning pathophysiology of pressure injury. Recent studies have revised the classical concept, showing that tissue pressures can become critical at levels inferior to conventional capillary closure pressure, depending on systemic influences.
Conclusions
Six case histories provide evidence that calf ulcers may be genuine pressure ulcers and lend support to the contemporary, comprehensive theory of pressure injury.
Pressure injuries represent a localized area of damage to the skin, soft tissue, muscle, or underlying tissues as a result of unrelieved pressure, especially where soft tissues are compressed between a bony prominence and any external surface [1, 2]. Decubitus provokes high interstitial pressures which deform and collapse the capillaries [3, 4], resulting in ischemia and hypoxia when lasting for a long time, and finally necrosis, i.e. pressure injury. The points of highest tissue pressure with the patient supine are at the sacrum, buttocks, heels and occiput, which are subject to pressures of 50-60 mmHg (5). The average capillary closing pressure, as measured by early investigators, is 30 - 32 mmHg [5]. Therefore, when the soft tissues at the sacrum, buttocks, heels or occiput are compressed to higher than capillary closure pressure for long periods of time, the resulting injury is called 'pressure ulcer', in keeping with tradition (1), or 'pressure injury' using the current definition [2]. Since interface pressures between the calf and the support surface in a supine person is 10 – 20 mmHg (as measured in the healthy male) and the capillary closure pressure approximates 32 mmHg, calf ulcers do not fit the classical concept of pressure injury.Calf ulcers are a common finding in practice and are due to various causes: venous insufficiency, vasculitis, metabolic disorders, neoplasia, infection, the effect of medications. On examination, the appearance of these ulcers differs from the appearance of pressure ulcers. Also different are the patients' clinical background and the features of the skin adjacent to the ulcer [6]. In distinction to the latter, several patients referred to our institution in post-acute care had calf ulcers that appeared to be pressure ulcers. The latter emerged in the absence of venous insufficiency, vasculitis, metabolic, or other recognizable causes of calf ulcers. To the clinician, the diagnosis ‘calf pressure ulcer’ was straightforward. Yet, perusing the literature under the key wards "calf, calves" AND "pressure ulcer, pressure sore, decubitus ulcer, bed sore, pressure injury" we could not find reference to calf pressure ulcers, except a recent reference of ours [7].
Case Histories
Our 210-bed institution includes facilities for rehabilitation, comprehensive nursing, and palliative care for elderly patients. During the 15 month period February 1st 2018 –30th April 2019, there were 1631 new admissions to our institution. Six patients had pressure ulcers on the calves. The patients' pertinent features are shown in Table 1. Brief case histories are presented next.

Case 1.
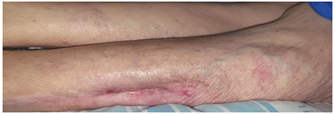
A 73-year-old woman was admitted to our institution for treatment of stage 3 pressure ulcers which developed during a 2-months hospitalization for bacterial endocarditis. Her medical history included numerous hospitalizations for schizoaffective disorder. She had been active and, until recently, able to perform two block walks. When admitted to our department in May 2018 she had completed the prescribed antibiotic regimen. Her body temperature and blood pressure were normal, the body mass index was 20.4. There was severe muscle wasting, most prominent of the calf muscles. A 3/6 pansystolic murmur was perceived at the cardiac apex. There were round, stage 3 pressure ulcers on typical locations: one in the lumbar area adjacent to the L1-L2 vertebrae, 6 cm in diameter, and three pre-sacral, the largest being 4 cm in diameter (Figure 1). On each calf there was a partially epithelized skin ulcer, respectively 20 cm and 22 cm long (Figure 2).


The hemoglobin was 10 g/dL, the MCV 97, serum albumin 3 g/dL, C reactive protein 0.8 mg/L. The patient received oral feeding 32 Kcal/kg and protein 1 g/kg body weight. Her daily medications were olanzapine 15 mg, lorazepam 1 mg, bisoprolol fumarate 1.25 mg, furosemide 40 mg, vitamin D 800 U, and enoxaparine 40 mg s.c. During an extended stay in our department her general condition was stable. The pressure ulcers were treated with saline gauze dressings changed every 6 hours; their non-inferiority vs. "advanced dressings" being documented [8, 9]. First to heal were the calf ulcers by December 2018 (Figure 3) followed 2-3 months later by the other ulcers. By February 2019 the size of the presacral ulcer had diminished by only 30 percent.
Case 2.
A 48-year-old man suffered a cardiac arrest at home. He was successfully resuscitated. Cardiac catheterization showed patent coronary arteries. Status epilepticus developed and he was transferred to neurology, received anticonvulsive therapy with partial suppression of the spells. He remained in vegetative state, had repeated pulmonary and urinary infections, and pressure ulcers developed during a 3-months hospital stay. When admitted to our department in August 2018 he was emaciated, the body mass index was 18.4 and muscle wasting was severe. There was a presacral pressure ulcer 9 cm in diameter with direct bone contact. A second pressure ulcer had developed in the vicinity of the right scapula, 4 cm in diameter, with deep pocketing and direct contact to ribs. A skin ulcer on the right calf, 14 cm long, 2.5 cm wide and 3 mm deep had granulation tissue at the base and a broad rim of new epithelium at the periphery. A skin ulcer on the left calf of similar size was completely epithelized. Among laboratory tests, remarkable were hemoglobin 11.4 g/dL, albumin 2.6 g/dL, C reactive protein 7.6 mg/L. He received enteral feeding through gastrostomy 35 Kcal/kg/day and protein 1.2 g/kg/day. The daily doses of medications were phenitoin sodium 200 mg, levetiracetam 1500 mg, insulin glargine and transcutaneous fentanyl 12.5 mcg/72 hours. The pressure ulcers were treated with saline gauze dressings and the adjacent dermatitis with antifungal crèmes. By February 2019 the calf ulcers were healed while the remaining pressure ulcers had only slightly improved.
Case 3
A 55-year-old man was transferred to our institution for end-of-life care. Recently he was found in narcotic overdose, deep coma, shock, aspiration pneumonia, respiratory and acute renal failure. He was mechanically ventilated and received antibiotic treatment. During prolonged hospitalization he had developed numerous pressure ulcers in the presacral area, the heels, ear and calves. On the posterior aspect of each calf there was a stage elongated skin ulcer: 18 cm long and 2 cm wide on the right calf, 13 cm long and 2 cm wide on the left calf. The patient did not recover from vegetative state and multiorgan failure. He died shortly after admission.
Case 4.
This 65-year-old man suffering from late onset familial muscular dystrophy had been ambulatory with the use of a walker. At home, he suffered a cardiac arrest. He was resuscitated and rushed to hospital in vegetative state from which he did not recover. He was mechanically ventilated. The hospital course was by complicated by the development of ventilator-associated pneumonia and urinary tract infections. Pressure ulcers emerged in the pre-sacral area, adjacent to the trochanters, scapula, shoulder, scalp, ear and calves (the diameters of the calf ulcers were 12 x 4 cm and 7 x 3 cm, respectively). He was mechanically ventilated and received enteral feeding through a nasogastric tube. His daily medications comprised 1000 mg sodium valproate, 75 mg metoprolol and 20 mg esmoprazol. He died 21 days after admission. No changes were apparent in the pressure ulcers during this time.
Case 5.
This 84-year-old man was admitted for rehabilitation after 29-day stay in hospital for pneumonia and cardio-respiratory failure. His medical history was notable for hemicolectomy, arterial hypertension and chronic atrial fibrillation. By the time he recently felt he was receiving anticoagulant prophylaxis with dabigatran. On admission a subdural hematoma was diagnosed, the anticoagulant treatment discontinued and intermittent pneumatic compression to the calves was instituted.
He continued treatment with daily phenytoin 200 mg, trazodone 50 mg, omeprazole 20 mg, and vitamin D 800 U. After two weeks pneumatic compression was replaced with enoxaparin 40 mg/day. A shallow ulcer had developed on the patient’s right calf. The calf ulcer healed 3 weeks later.
Case 6.
A 90 year-old woman, living in the community was hospitalized with aspiration pneumonia and acute respiratory failure. Mechanical ventilation was initiated. Her medical history included myocardial infarction, diabetes mellitus, arterial hypertension, atrial fibrillation and venous thromboembolism. During hospitalization she developed ventilator-associated pneumonia, shock and acute renal failure. Anticoagulant treatment was temporarily discontinued and intermittent pneumatic compression was applied to the calves until the renal function improved and heparin sodium was initiated. Following unsuccessful trials of weaning from mechanical ventilation she was transferred to our institution for long-term life support. She was alert and hemodynamically stable. A stage 3 skin ulcer was present on her left calf, 10 x 4 cm in diameter, with a rim of new epithelium at the periphery (Figure 4).

There were no other skin ulcers. Notable among the laboratory tests were hemoglobin 8.5 g/dL, serum albumin 2.5 g/dL and eGFR 42 mL/minute. The patient's medications were lercanidipine 20 mg/day, esmoprasole 20 mg/day and heparin sodium. Under treatment with saline gauze dressings the calf ulcer healed.
Discussion
The calf ulcers in the six patients differed from venous, ischemic, neuropathic and stasis ulcers as well as from vasculitic, metabolic, infectious, neoplastic skin ulcers, pyoderma gangrenosum and calciphylaxis [1, 2, 5]. Except for their elongated shape, contrasting to the round shape of pressure ulcers at other sites, the calf ulcers in the six patients were similar to typical pressure ulcers [1, 2]. In the six patients the calf ulcers appeared alike the ‘typical pressure ulcers’ except for their elongated shape. Alike typical pressure ulcers their borders were regular and well demarcated, and the adjacent skin appeared normal. Alike typical pressure ulcers, the calf ulcers occurred in hospital during an acute severe illness. In four patients the calf ulcers occurred concurrently with the typical pressure ulcers. In the patients described as Cases 1-4, the pressure ulcers appeared under multisystem deterioration (shock, sepsis, hypoxia, multiorgan failure) along with exposure of the skin to local injury. These four patients developed numerous, bilateral pressure ulcers, both calves involved, in what appeared to be “systemic" pressure injury. The clinical picture may be in extremis that described as "Kennedy Terminal Ulcer", characterized by rapid onset and rapid tissue breakdown [10]. At difference, patients described under Case 5 and Case 6 developing but one calf ulcer and no further pressure injury. The cause of the “locally limited" pressure injury in these two patients appeared to be local, related to the use of intermittent pneumatic compression for thromboprophylaxis. Indeed, skin breaks [11] and rarely pressure ulcers [12] belong to adverse effects of intermittent pneumatic compression. Hence, calf ulcers may be part of systemic pressure injury or the result of locally limited damage. Underreporting of calf pressure ulcers might be due to the conflict between bedside observation and the ischemic concept of pressure injury. Their development cannot be explained by the classical theory of pressure injury since interface pressures on the calves were thought not reaching the capillary closing pressure of 30-32 mmHg. Recently, the pathophysiology of pressure injuries was revised based on MRI and digital fluorescent microscopy studies. Misconceptions were identified [13]. First, under weight-bearing and immobility the capillaries in the affected tissues are not completely occluded but stay, at least partially, open [14]. Second, the correlation between interface pressures and internal tissue pressures is weak. Since stage 3 and 4 pressure injuries begin in the deep tissues, the 32 mmHg "ischemia threshold" measured in superficial capillaries might be misleading [13,15]. Third, sustained tissue deformation caused by body weight damages the integrity of cells while pressure applied in excess does not necessarily cause ischemia. Cell membrane buckling and rupture alters the transmembrane transport of biomolecules and ions, causes volume changes and alters the cytoskeleton, affecting cellular viability. Apoptosis and cell death may ensue [16]. Ischemia adds to the severity of tissue injury several hours after injury has been caused by tissue deformation [17, 18]. Fourth, systemic factors might be crucial in modifying tissue tolerance to deformation and ischemia. Hypotension, blood flow redistribution, damage by proinflammatory cytokines, acidosis and electrolyte disturbances might impact the tissues' tolerance to ischemia. Persistent alterations of the microcirculation despite restoration of macro-hemodynamics and reperfusion injury during removal of pressure load can add to tissue injury [19]. There is no fix value of tissue pressure above which injury develops, rather different levels of tissue pressure can become critical depending on systemic and local influences [20]. External pressure alone might not suffice to cause a pressure injury. Rather, interaction of local forces with systemic alterations lead to tissue damage. Hence, it is not surprising that most pressure ulcers emerge during hospitalization for acute severe illness [2] as a part of the multiorgan system failure.
Six case histories provide evidence that calf ulcers may be genuine pressure ulcers as part of systemic pressure injury or as a limited local damage. Observations at bedside lend support to the recent, broadened understanding of the pathophysiology of pressure injury.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
